Cognitive behavioral therapy (CBT) is a form of psychological treatment that has been demonstrated to be effective for a range of problems including depression, anxiety disorders, alcohol and drug use problems, marital problems, eating disorders, and severe mental illness. Numerous research studies suggest that CBT leads to significant improvement in functioning and quality of life. In many studies, CBT has been demonstrated to be as effective as, or more effective than, other forms of psychological therapy or psychiatric medications.
There are many types of modalities or techniques used in CBT, but the technique used to treat Anxiety and Anxiety Spectrum Disorders like OCD among others is Exposure-Response Prevention (ERP). ERP is the gold standard treatment model and is excellent when enhanced or integrated with other therapies like Mindfulness, which includes Acceptance and Commitment Therapy (ACT). Regardless of the integration of other therapies into the mainframe treatment, ERP must be a part of the foundational therapy. The basic principles of ERP include the following:
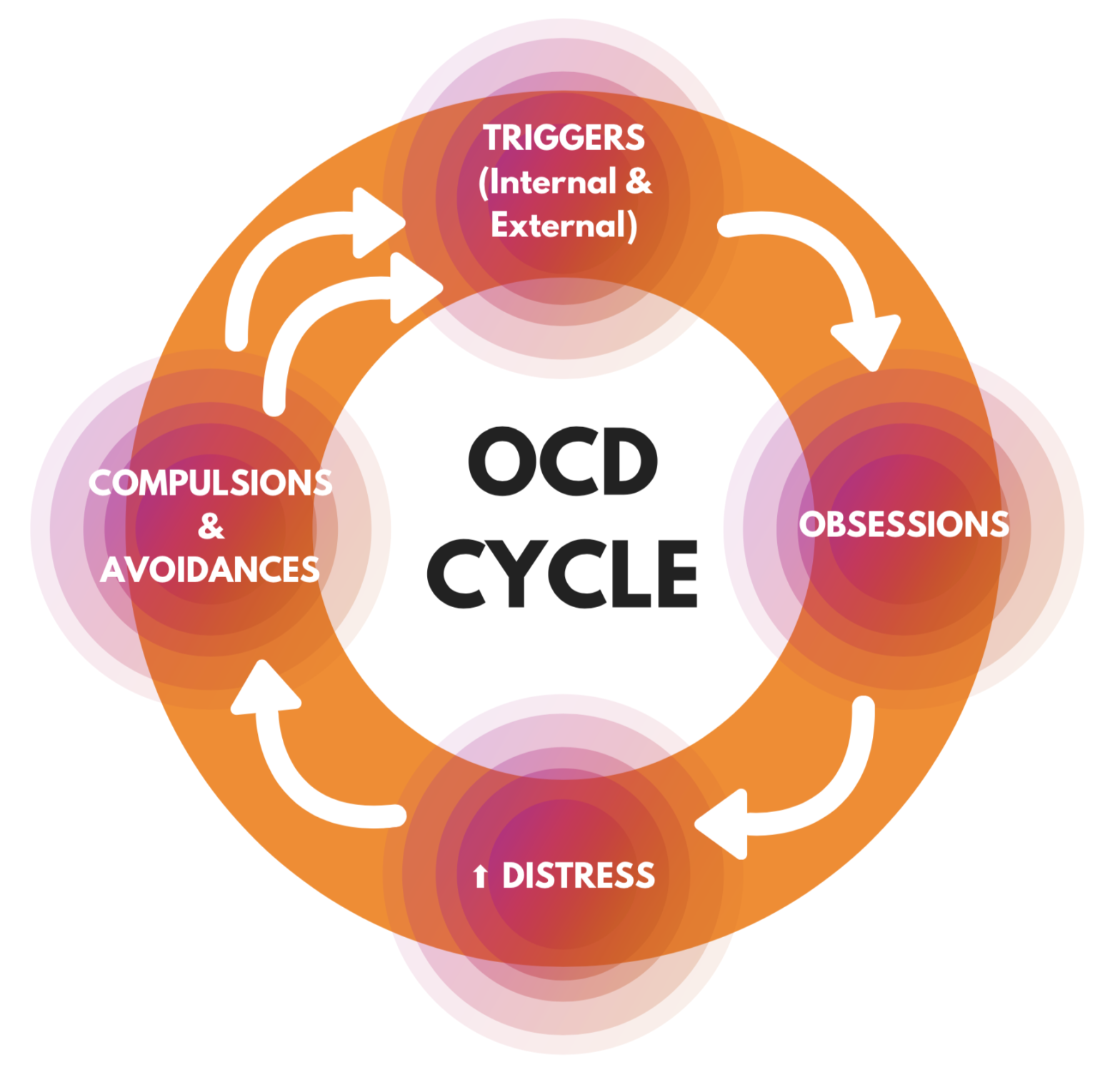
- Obsessions, Compulsions, triggers, and safety behaviors are identified and ranked in terms of distress.
- Clients will be exposed to feared situations or images related to their obsessions which will elicit anxiety.
- Clients are instructed to avoid the compulsive behaviors, rituals, and safety behaviors (hence response prevention part of the treatment name).
- The client must stay exposed to the anxiety provoking situation, while witnessing that nothing terrible is happening as a result of not trying to control, prevent, or alter the feared outcome.
- The mind and body will learn that thoughts are just thoughts and not necessarily reality, which helps the nervous system and mind develop a healthier thought-response pattern.
- Anxiety due to the specified trigger will shift as exposures are repeated and no compulsions, rituals, or safety behaviors are engaged in.
Clients will learn that they can cope without relying on trying to alter, change, or control circumstances and that whatever comes up can be dealt with without engaging in those compulsions, rituals, or safety behaviors. Even if anxiety does come around it, it can be better managed.